| ANAESTHESIA PEARLS |

| ||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||
| Perioperative laryngospasm is an anesthetic emergency that is still responsible for significant morbidity and mortality in pediatric patients. | ||||||||||||||||||||||||||||||||||
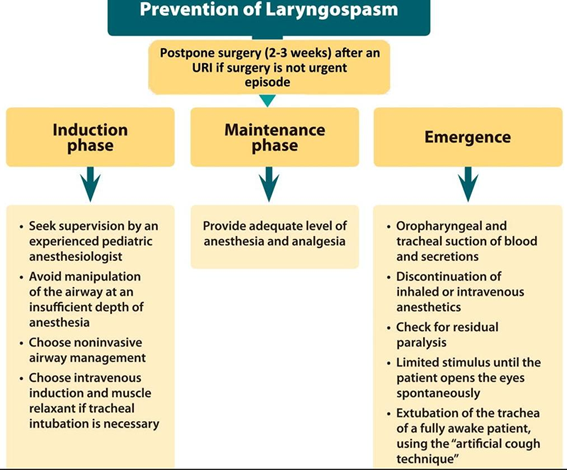
| The first step of laryngospasm management is prevention. | ||||||||||||||||||||||||||||||||||


 |
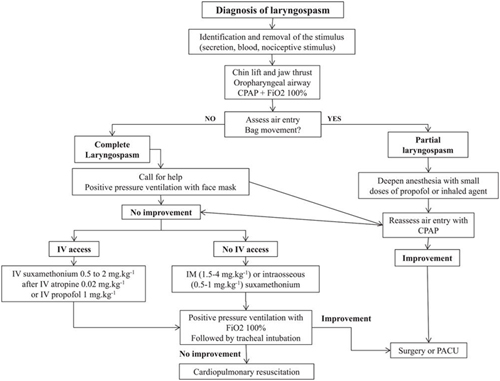
The second step relies on the emergent treatment of established laryngospasm occurring despite precautions.
Training and simulation on the management of laryngospasm in children:
Supplemental Digital Content
| ||
|
||
 | ||
Laryngospasm is the most common cause of upper airway obstruction after tracheal extubation. Magnesium has a central nervous system depressant property, which contributes to the depth of anaesthesia. It also has calcium antagonist properties, which provide muscle relaxation. | ||
To determine the effect of magnesium on preventing laryngospasm, 40 patients, ASA I–II, aged 3–12 years, who were scheduled for tonsillectomy or/and adenoidectomy, were randomly divided into two groups. | ||
After intubation, patients in group I received 15 mg•kg−1 magnesium in 30 ml 0.9% NaCl over 20 min. Patients in group II received 0.9% NaCl alone. | ||
All patients were extubated at a very deep plane of anaesthesia. | ||
Laryngospasm was not observed in group I, it was observed in five patients in group II (25%) | ||
This study concluded the decrease in the incidence of laryngospasm in paediatric patients receiving magnesium. | ||
It is suggested that the use of intravenous magnesium intraoperatively may prevent laryngospasm. | ||
Ref: | ||
|
||
This method involves the application of digital pressure at the “laryngeal notch”. | ||
This notch is located behind the lobule of the pinna of each ear. It is bounded anteriorly by the ascending ramus of the mandible adajacent to the condyle, posteriorly by the mastoid process of the temporal bone and cephalad by the base of the skull. | ||
 | ||
The therapist presses very firmly inwardly toward the base of the skull on each side using either the index or middle fingers while at the same time lifting the mandible at a right angle to the plane of the body (forward displacement of the mandible or jaw thrust). | ||
 | ||
Paediatric unilateral | ||
Properly performed, it will convert laryngospasm within one or two breaths to laryngeal stridor and in another breath or two to unobstructed respiration. One can simultaneously hold the mask over the face with the thumbs to augment the inspired oxygen concentration. | ||
| ||
Adult bilateral | ||
Why does it work? | ||
It's unclear about the mechanism behind why this works. Here are some theories: | ||
You are just performing a jaw-thrust maneuver. |
||
You are providing a deep painful stimuli, which causes the vocal cords to relax. | ||
You are stimulating deep cranial nerves which happen to also stimulate the vagus nerve. | ||
Bending the styloid process and producing periosteal pain is another explanation | ||
Ref: | ||



